
Study
The rate of COVID-19 vaccination in Israel is one of the highest in the world. However, vaccine rates are not evenly distributed among the different population groups. Arab citizens and the Ultra-Orthodox population, who have suffered the most from the pandemic, are vaccinated at lower rates than the general public. Moreover, social media disinformation campaigns that have characterized the COVID-19 pandemic in Israel, in general, and the vaccine, in particular, has been one of the causes of vaccine hesitancy.

This study is part of the series "No one is safe until everyone is safe - Global perspectives on Covid-19 vaccination" by the Heinrich-Böll-Stiftung's European Union and Washington, DC offices.

Download the study "Global perspectives on Covid-19 vaccination - Access to the Covid-19 vaccine in Israel" by Shelly Kamin-Friedman
State of the COVID-19 pandemic in Israel
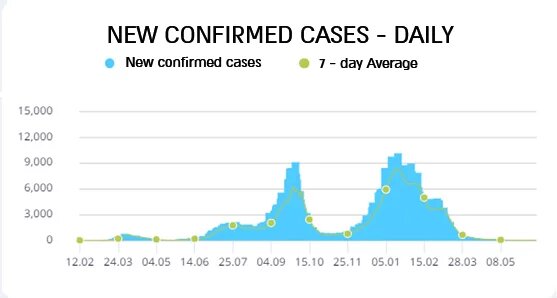
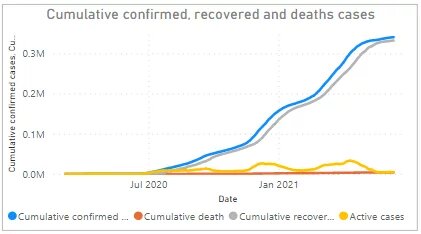
Israel has confronted three "waves" of the COVID-19 pandemic thus far. The first wave began after the identification of Israel’s first COVID-19 carrier on 27 February 2020. The carrier was an Israeli citizen who returned from Italy three days earlier [1].
An exponential increase in the number of confirmed cases led to a full lockdown, which was imposed on 7 April 2020, for a period of three days. People were prohibited from being more than 100 meters away from their place of residence, except in order to buy food and/or medicine. The public complied with the provisions of this tight lockdown and morbidity decreased [2].
However, following the reopening of the economy the number of confirmed carriers and seriously ill patients began to rise again. The sharp increase in morbidity was followed by a second full lockdown on 18 September 2020 [3].
After the first two waves, the Ministry of Health recommended that the economy be re-opened in stages based on health indices, with 14 days elapsing from one stage to the next. However, the Ministry's recommendations were not implemented in practice. The stages for reopening the economy were advanced, and the number of confirmed cases began to rise again, especially in Arab localities.
https://datadashboard.health.gov.il/COVID-19/general (14 June 2021) [5]
A vaccination campaign began in Israel on 19 December 2020, following approval by the U.S. Food and Drug Administration (FDA) of the Pfizer vaccine [4]. Nevertheless, the daily number of confirmed cases and deaths continued to rise.
On 27 December 2020, the government resolved to impose a third lockdown, which included the shutdown of commerce, the imposition of restrictions on workplaces and the partial operation of the education system. Even so, the increase in morbidity and mortality continued.
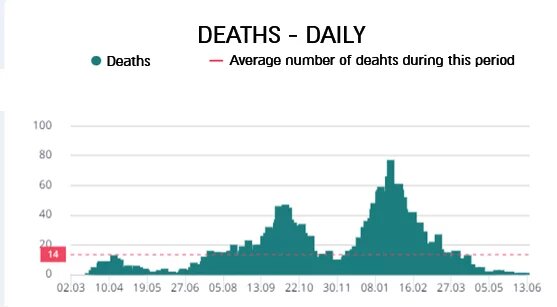
https://datadashboard.health.gov.il/COVID-19/general (14 June 2021) [5]
In February 2021, when 34.98% of the population had been vaccinated with the first dose and 20.26% with both vaccine doses [5], a slow decline began in the number of daily confirmed cases, the number of seriously ill patients and the number of deaths. On 10 March 2021, the infection coefficient (R) reached 0.9, marking a halt in the spread of the virus [5]. The economy opened up, and Israel returned to almost complete normality as the rate of vaccination increased and the rate of morbidity decreased.
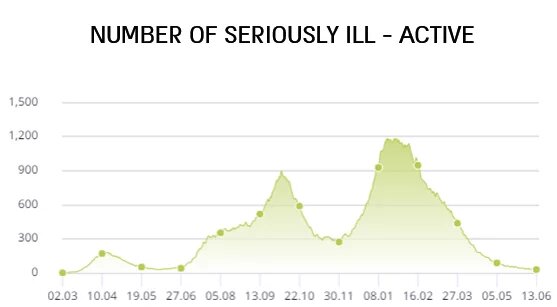
https://datadashboard.health.gov.il/COVID-19/general (14 June 2021) [5]
Current state of vaccine deployment in the country
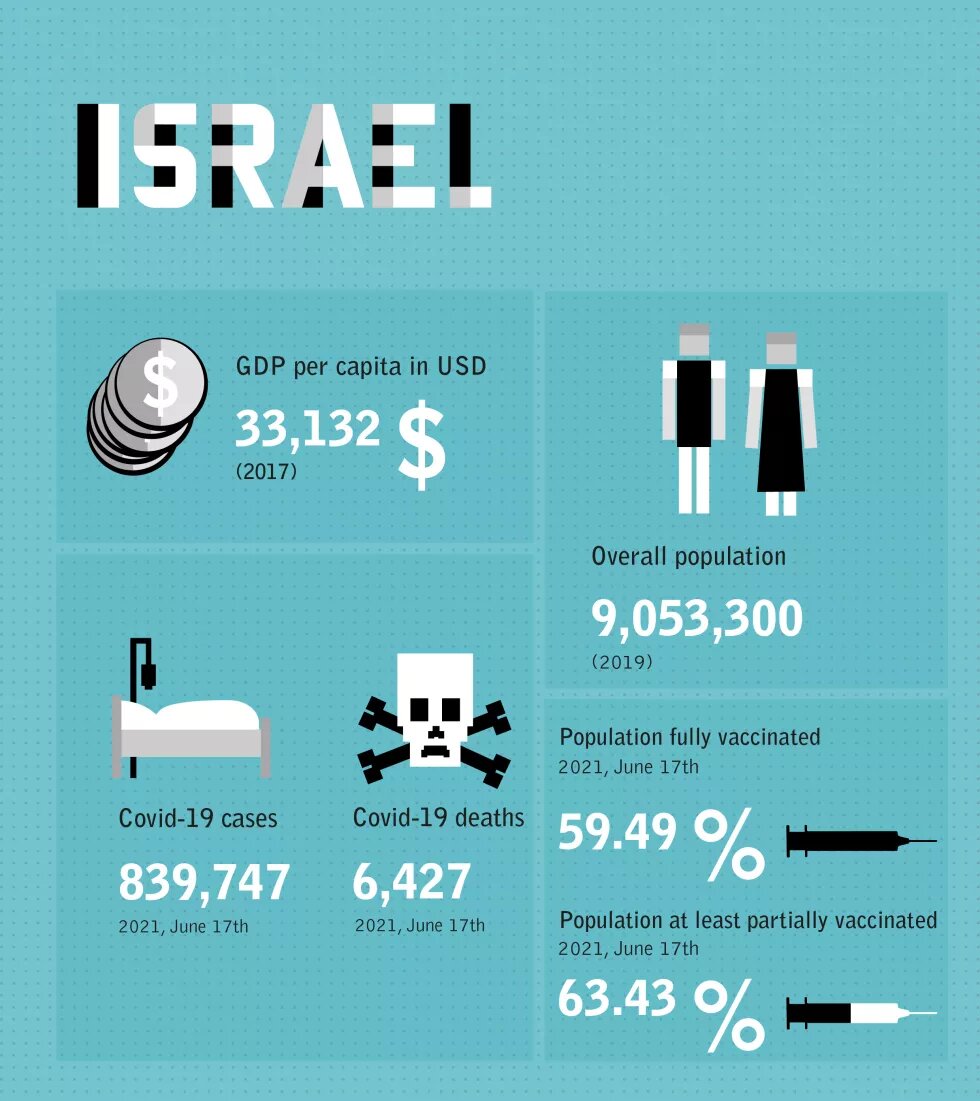
As noted above, Israel’s vaccination campaign began on 19 December 2020, approximately one week after the FDA granted emergency approval for the Pfizer vaccine (BNT162b2) [6]. At the time of writing (14 June 2021), almost four months after the vaccination campaign began, 5,476,317 people have been vaccinated with the first dose, and 5,144,382 with both doses. In the age group over 90, 94.6 % of the population were vaccinated, in the next age group ranging from 80 to 89 years 93% were vaccinated, in the age group 70-79 years 95.4 %, in the age group 60-69 years 86.6%, and in the age group 50-59 years, 84.6 % were vaccinated. When examined comparatively, the number of vaccinees in Israel is among the highest in the world.
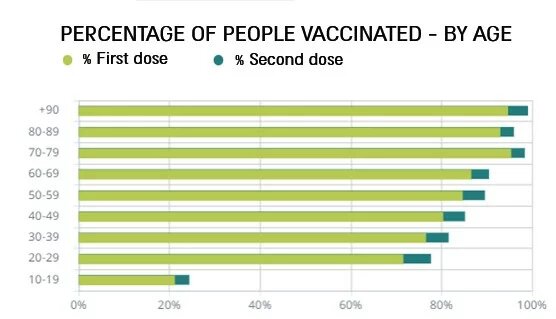
https://datadashboard.health.gov.il/COVID-19/general (14 June 2021) [5]
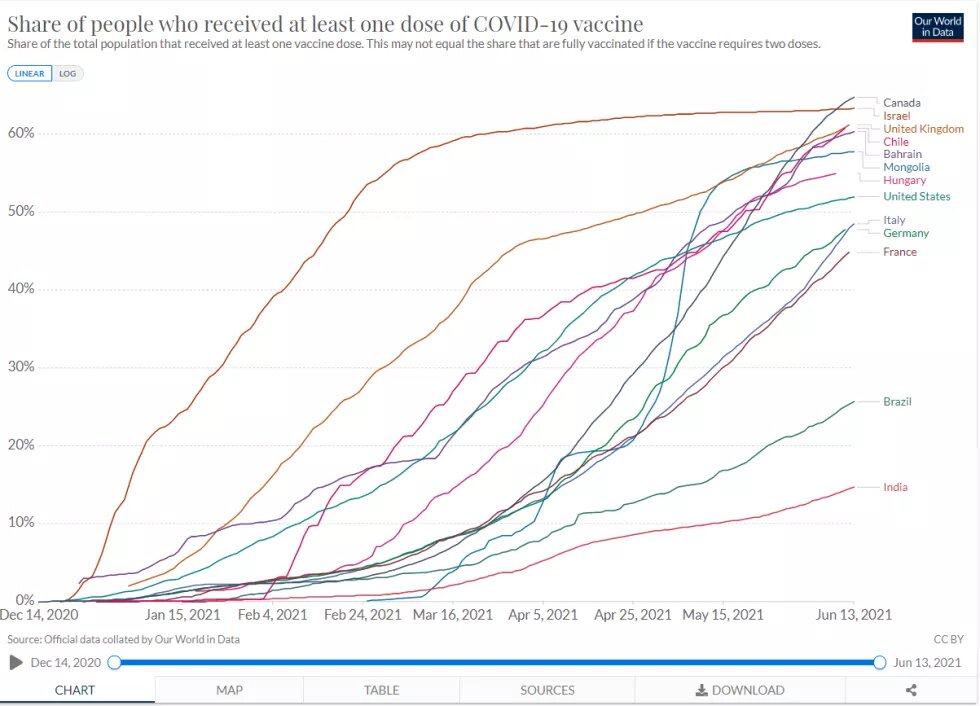
https://ourworldindata.org/covid-vaccinations (14 June 2021) [9]
Nonetheless, vaccine rates are not evenly distributed among the different population groups. Arab citizens and the Ultra-Orthodox population, who have suffered the most from the pandemic, are vaccinated at lower rates than the general public.
BriLife, a vector-based Israeli vaccine
The Israel Institute of Biological Research (IIBR) has been working on the development of an Israeli vaccine as part of Israel’s efforts to curb the spread of COVID-19. BriLife is a vector-based vaccine that takes Vesicular stomatitis virus (VSV) and genetically engineers it to express the spike protein of the SARS-CoV-2 beta coronavirus on its envelope [7].
The refrigeration required to transport the vaccine (2-8 degrees Celsius) is much more convenient than the refrigeration required for mRNA vaccines, and its cost is therefore expected to be lower than that of the Pfizer vaccine.
BriLife’s development, financed by the State of Israel, is currently in Phase II after no significant side effects were found in Phase I. The current phase includes extensive safety tests on some 1,000 volunteers, and is being managed by an American biotechnology company IQVIA [8].
The high outlays involved in the development of BriLife have triggered public criticism. One argument asserts that by the time an Israeli vaccine is approved, provided that the clinical trials are successful, the country’s population will have been largely vaccinated. Another argument asserts that the IIBR was created to address security threats and that it operates under a shroud of secrecy. Information on the progress of the vaccine development is therefore confidential and not disclosed to the public. Critics also mentioned an experiment previously conducted secretly by the IIBR as part of the development of an anti-anthrax vaccine, an experiment that was performed on soldiers in a manner that did not comply with the principles of the Helsinki Declaration [9].
The clinical trials conducted with the Israeli vaccine have also encountered ethical difficulties. A question was raised regarding whether the trial participants could be regarded as immunized against the virus in the same way as people who were vaccinated with the Pfizer vaccine, in spite of the fact that the effectiveness of the Israeli vaccine has not yet been proven and given that some participants actually received a placebo [10]. The legislation making admission to public or business locations contingent on the presentation of a Green Pass stipulates that participants in the Israeli clinical trial are entitled to such a pass in the same manner as “recovering” individuals or individuals vaccinated with the Pfizer vaccine [11].
Which vaccines are used and who provides them?
Alongside the effort to develop an Israeli vaccine, the State of Israel signed APAs (Advanced Purchase Agreements) with Moderna [12], Pfizer [13], and AstraZeneca [14], when all three vaccines were in phase III of clinical research and before they had received FDA approval.
FDA approval for the Pfizer vaccine was granted on 11 December 2020, and Israel’s vaccination campaign began on 19 December 2020. The vaccinations were administered by health maintenance organizations (HMOs), hospitals and Magen David Adom (MDA), also known as the Israel Rescue Organization, which is responsible for vaccinating the residents of nursing homes and assisted living facilities.
Israel’s success in gaining a rapid supply of vaccines is credited to its general characteristics and to the unique qualities of its healthcare system [13]. The fact that it is a small country facilitated the transport of vaccines to remote localities under the required refrigeration conditions. The fact that the population is relatively young (only 12% over the age of 65), in turn allowed for the rapid vaccination of the population at risk, and the mild weather in December 2020 made it easier for elderly people to report to vaccination centres. As for the healthcare system, Israeli law [15] requires every resident to belong to one of four non-profit HMOs. These maintain computerized records on every member, including age and health risks, and thus facilitate the tracing of at-risk populations as well as the targeted efforts to get them vaccinated [16].
HMOs have long been prepared to handle an unusual biological event and are skilled in the rapid deployment of vaccination centres around the country. In addition to their nationwide network of clinics, HMOs also opened combined vaccination centres in peripheral areas, and medical staff vaccinated housebound people in their homes. HMO vaccination appointments were made by phone, or via their websites or mobile phone applications, and a national record-keeping apparatus helped in tracking the number of vaccinees and side effects [13].
In order to prevent vaccines from going to waste after they were removed from refrigeration, each 1,000-dose tray was ingeniously split into smaller containers that were transported to remote areas with a low number of potential vaccinees. In addition, vaccines left behind due to “no shows” were offered to people who had not yet reached their turn to be vaccinated according to the prioritization rules. This measure led to a certain degree of vaccination inequality (digitally literate young people, as opposed to other groups, easily identified vaccine centres where excess vaccines were available), but this inequality was very short-lived given that the vaccines were soon offered to the entire population.
When were COVID-19 vaccines approved in Israel?
The FDA approval for the BNT162b2 vaccines was followed by deliberations of Israeli health experts, who recommended the administration of the vaccine in Israel. Nonetheless, it should be noted that the BNT162b2 vaccines have not yet been registered in the Ministry of Health’s Drug Directory. Israeli law stipulates that the sale of a therapeutic or prophylactic drug is conditional on such registration, but it makes an exception for drugs imported from overseas in order to protect Israel’s residents from an epidemic disease 17]].
Why was a certain vaccine chosen over others?
The APAs signed with Pfizer, alongside the ability of delivering the vaccines to the public, led to Pfizer’s decision to advance its shipments to Israel. A further consideration taken into account with regard to this decision was Israel’s well-developed electronic health records, and their importance for studying the vaccine in real world situations cannot be overstated. Israel committed to sharing epidemiological data with Pfizer, such as the number of vaccinees, vaccine side effects, vaccine efficacy and the time elapsing until the development of antibodies. In response to the fears expressed about an invasion of privacy concerning vaccinees, the Ministry of Health clarified that no personally identifying information would be transferred to Pfizer, but rather aggregate data alone [18].
The continuous supply of BNT162b2 vaccines has allowed Israel to vaccinate the entire population over the age of 16 via the same method (two vaccine doses, a compound mixed with NaCl, 5-6 servings per vial) without overloading the relevant operational systems. Some 100,000 Moderna vaccine doses shipped to Israel were kept as a reserve in case Pfizer’s continuous supply ceased 19]].
Are vaccines free of charge for the whole population?
The vaccines were purchased exclusively by the state, financed by public funds and provided free of charge to all inhabitants. People living in Israel who do not satisfy the definition of “a resident”, such as foreign workers or asylum seekers, are also entitled to free vaccination, although their eligibility for vaccination was approved belatedly, and only after the at-risk citizens had been vaccinated [20].
In spite of its public funding, vaccination response rates have been lower in less affluent localities compared to affluent localities [21] as well as lower in Arab localities compared to Jewish ones [5] [22].
Which timeline will vaccinations follow, and when are vaccines expected to be widely available to the general public?
The Ministry of Health laid down the principles of prioritization shortly before the commencement of the vaccination campaign (in December 2020): health and epidemiological urgency, safety, simplicity, breadth, flexibility, and efficiency in order to ensure vaccine effectiveness and efficacy. Priority was given to medical staff, nursing homes for the elderly and their caregivers, and people over the age of 60 living in the community. It was noted that flexibility should be exercised and that the caregiver of an elderly person in the community should also be vaccinated. A slightly lower priority was given to at-risk groups (diabetics, morbidly obese individuals, individuals suffering from COPD, individuals with hypertension, immunosuppressed patients, the recipients of organ transplants, haematology patients, etc.), and high-exposure groups (school and kindergarten teachers, social workers, prison inmates and wardens, and first responders) [23].
Contrary to the prioritization rules, the Minister of Public Security ordered the Israel Prison Service to refrain from vaccinating prisoners until he gave his approval depending on the progress of the general vaccination campaign 24]]. In response to a petition filed by Physicians for Human Rights-Israel (PHR) and other human rights organizations, the Supreme Court ruled that prisoners have a legal right to medical treatment, including vaccines, and noted that the crowded conditions in prisons and the impossibility of isolating inmates suspected of having contracted the SARS-CoV-2 virus increase the risk of morbidity and mortality and requires the prioritization of inmate vaccinations, especially those given to prisoners over the age of 60 and those with pre-existing medical conditions [25].
It was recommended—at least initially—that individuals who had recovered from COVID-19, pregnant women, lactating women, people with a history of severe anaphylaxis, women planning to become pregnant, and children and adolescents up to the age of 16 should not be vaccinated [23]. However, the guidelines were updated on 23 December 2020, to state that pregnant women could be vaccinated if they so wished. The contraindications to vaccinating patients with a history of allergic reactions were similarly updated (vaccination would only be avoided in cases where anaphylaxis occurred in response to one of the vaccine components, in response to certain drugs administered by injection or due to idiopathic reasons) [26].
The guidelines pertaining to the vaccination of pregnant women were updated once again on 28 January 2021. This time, the guidelines affirmed that vaccination was in fact recommended for women planning a pregnancy, women in the second or third trimester of pregnancy and breastfeeding women [27]. In addition, and in order to promote the reopening of the education system, the government also resolved to add students over the age of 16, as well as school and kindergarten teachers, to the highest priority group.
As the vaccination campaign progressed, the age of eligibility for vaccination gradually decreased, and the government eventually resolved to extend the vaccination campaign to the entire population over the age of 16 in February 2021 [28].
Nonetheless, there is some controversy surrounding the need to vaccinate children between the ages of 12 and 15 in order to control the spread of the virus. The health ministry experts deliberated the issue, following the recent FDA approval to vaccinate this age group. Meanwhile, some 618 young children with an increased risk of COVID-19 complications have already been vaccinated with the approval of the Exceptions Committee, and no side effects have been reported thus far [29].
What are the expected consequences of the vaccine deployment for the economic outlook in Israel?
The impact of a high degree of vaccination compliance on Israel’s economy can be gleaned from a January 2021 comparison between two economic forecasts: one based on a rapid vaccination campaign completed by May 2021, and another based on a slow vaccination campaign that would last throughout 2022 [30].
The rapid vaccination scenario predicts a total growth rate of 6.3% by the end of 2021 as the removal of restrictions will trigger a relatively quick recovery that will continue throughout the second quarter of 2021. However, due to the loss in income suffered by businesses and households, economic activity will not return to normal levels and an additional lengthy process will be required to attain that objective. As a result, the level of activity in 2022 will be approximately 2% below the long-term GDP trend. In the slow vaccination scenario, on the other hand, the growth rate is predicted to be a mere 3.5% by the end of 2021. The gap can mostly be ascribed to the possibility of new lockdowns, a state of affairs that exerts severe harm on private consumption.
In April 2021, the Bank of Israel announced that it would, in light of the progress in the vaccination campaign and the decline in morbidity, henceforth focus its macroeconomic forecast on the rapid vaccination scenario (6.3% growth in 2021). Israel’s central bank also predicts that morbidity will not rise significantly until the end of the year and thereby obviate the need for reinstituting restrictions with weighty economic implications [31].
Cultural and socio-political implications regarding vaccine acceptance
Do people trust or distrust the vaccine with regard to its safety, and are they more worried about the virus or the vaccine?
The coronavirus vaccination campaign in Israel was initially characterized by a volume of demand that exceeded the HMOs’ daily supply, and at the time of writing (14 June 2021), a large percentage of the at-risk population had already been vaccinated. However, the rate of compliance among this group and among the general public has yet to reach 100% (for example, only 84.6 % of individuals aged 50-59 have been vaccinated thus far) [5]. Compliance rates have also been relatively lower among the Arab population compared to the Jewish population in Israel and among women compared to men [32].
In general, “vaccine hesitancy” in Israel has not been ascribed to a lack of knowledge, but rather to a surfeit of knowledge. Israeli vaccine sceptics feel conflicted between the benefit of vaccination and the risk of illness. Given that conflict resolution is a proactive step, laypeople choose not to rely on the recommendations of others and would rather make their own decisions. This reflexive approach, in turn, derives from Jewish tradition, where questions are part of the learning process. In addition, the State of Israel’s short history is full of rifts, a diversity of opinions and a lack of trust in the authorities. These are fertile ground for a climate of scepticism with respect to the recommendations made by the health authorities [33].
When examining the reasons for COVID-19 vaccine hesitancy in Israel, the most common appears to be concern about the rapid development of a new vaccine whose long-term consequences are yet to be known. A study conducted prior to the vaccination campaign showed that the issue of the risk posed by the vaccine was a factor that influenced the decision to get vaccinated – even among medical personnel [34]. Another reason was disinformation campaigns propagated on social networks [35].
The relatively low rate of vaccination compliance among the Arab public can be explained by the socioeconomic discrimination of the Arab population in a variety of domains, including differences in the amount of resources allocated to the informational campaigns about the dangers of COVID-19 deployed for the Jewish and Arab publics, respectively [36].
Another explanation for the low rate of vaccination compliance in Arab society is the lack of trust in the health system and in the state establishment itself; this stems from, among other things, the poor handling of the COVID-19 crisis in Arab localities. Furthermore, the prioritization rules (which favoured people over the age of 60) were out of step with Arab demographics, which are characterized by a relatively young population. A relatively low rate of digital literacy has also made it difficult for elderly persons to make vaccination appointments online and not enough efforts were devoted to reaching this population or to helping them travel to the vaccination centres [37] [38].
Is vaccination mandatory?
COVID-19 vaccinations in Israel are optional rather than mandatory. However, in order to promote compliance and to allow the safe reopening of the economy, a law was passed that made admission to some businesses and public places contingent on the presentation of a Green Pass. This is a certificate issued by the Ministry of Health indicating that its holder has recovered from COVID-19, has been vaccinated or is a participant in the clinical trial associated with the development of an Israeli vaccine.
The businesses and public places whose openings had been approved for Green Pass holders only include gyms or fitness studios, venues where cultural activities or sporting events take place in the presence of an audience, venues where exhibitions are held, hotels, swimming pools, banquet halls and gardens, restaurants, and tourist attractions. According to the regulations, the operators of a public or business place where admission is contingent on the presentation of a Green Pass may place a rapid COVID-19 test (which does not require analysis by a laboratory) station at the door. A negative result in such a test would only admit individuals to that specific place alone.
Arguments against the Green Pass requirement as a tool for promoting vaccination compliance include the negative labelling of people who refrain from vaccination, the harm inflicted on public trust due to the use of coercive legislation, deepening social disparities due to the lower vaccination accessibility of disadvantaged populations, and the fear of expanding the range of rights which may only be exercised subject to vaccination. However, the general consensus was that the demand to produce a Green Pass to gain admission to businesses and public places would promote the reopening of the economy and would represent a calculated risk with respect to harming the efforts to control the pandemic [39].
The Israeli legislation refrained from requiring a Green Pass in places where admission is essential to the exercise of individual rights: hospitals, clinics, pharmacies that are necessary for exercising the right to health, and houses of worship that are necessary for exercising the freedom of worship. Public places that include businesses providing both essential services and leisure activities (such as shopping malls) were opened to the public without restrictions.
What is the vaccination status of the population with respect to other diseases that might serve as examples?
The rate of COVID-19 vaccination in Israel is one of the highest in the world. The rate of compliance has also been impressive compared to previous vaccination campaigns during earlier outbreaks of infectious diseases. For example, when the swine flu pandemic erupted in 2009, the vaccination rate was only 12% [40]. When poliovirus was discovered in the sewage system in 2013 and the health authorities resolved to administer oral vaccines (OPV) to people born from 2004 onwards, the average compliance rate was around 80% nationwide, but only 64% among children in and around Tel Aviv.
The high rate of compliance with the COVID-19 vaccine compared to the flu and poliovirus vaccines should be credited to the Ministry of Health and to Israel’s HMOs, who both made the vaccines physically accessible to the general population, as well as to advocacy efforts by medical teams and public influencers on all media outlets and social networks.
Having said that, the vaccination rate for the routine vaccines recommended for children is higher; for example, the rate of vaccination against measles, mumps, rubella and varicella [MMRV] is 96%, and 95.2% against diphtheria, tetanus, pertussis and polio (DtaP+IPV), but a vaccine against the HPV (Human Papilloma Virus) introduced in 2013 experienced a compliance rate of only 49.3% (with respect to the two vaccine doses required) [41]. The lower response to HPV vaccination can be attributed, among other things, to fear about possible adverse effects [33], which also characterizes the COVID-19 vaccine.
Is disinformation about vaccines a relevant factor?
As noted above, the social media disinformation campaigns that have characterized the COVID-19 pandemic in Israel, in general, and the vaccine, in particular, has been one of the causes of vaccine hesitancy. The fact that the development of the vaccine was completed within a year, and the fact that there are no definitive answers regarding its long-term effects, thus far leaves much room for intimidation and speculation [34].
Among other things, fake news was spread to the effect that the vaccine would lead to systemic collapse within six months due to Antibody-Dependent Enhancement (ADE), that it was not approved for use and did not pass the required tests, and that it changes vaccinees’ DNA and causes more severe morbidity and greater mortality than COVID-19 itself. In the Ultra-Orthodox population, social media was rife with disinformation about the link between the vaccine and infertility. In this respect, it should be noted that fertility and childbearing possess a great deal of social and cultural importance in Israel. In the Arab sector false news has spread that the vaccine administered to Arabs is expired.
In an attempt to deal with fake news, the Ministry of Health launched an informational campaign and a dedicated website that provided professional answers to all relevant questions [42]. In addition, ministry-appointed social media analysts detected untruthful posts, which doctors checked and posted on-the-spot rebuttals. Jurists examined whether the posts constituted a misdemeanour under the Computer Law, and, if this was indeed the case, filed an official request on behalf of the State of Israel with the pertinent social network asking for the bogus content to be removed.
Following a request from the State Attorney’s Cyber Affairs Department, Facebook removed four groups that had posted reports and videos containing false and misleading information (one of the groups reportedly encouraged members to set appointments but not to show up in order for vials to go to waste and thus deprive people of vaccines). The request sent to Facebook noted that the false publications could pose a real danger to public health as readers exposed to the information might erroneously believe that they were truthful and would thus shun vaccination. However, groups removed from the network often reappeared the next day under a slightly different name and with the same number of followers [43].
Special attention was also paid to the false news in Haredi (Ultra-Orthodox Jewish) society that was published in pashkevils (neighbourhood bulletin boards). The Ministry of Health published counter-pashkevils, but these were torn down and once again replaced by false ones [44]. On the other hand, fake news in Arabic to which Israeli Arabs were exposed received no special attention, and the Ministry of Health only recruited Arab doctors to help disseminate reliable information about vaccines at a relatively late stage [45].
Expectations from international actors
What are the expectations in your country from other international actors, such as those involved in COVAX?
As noted above, the State of Israel is among the world’s leading countries with respect to the progress made in COVID-19 vaccination. However, the Palestinian population in the West Bank and Gaza Strip (unlike the Arab citizens of Israel), has been left behind and depends on the assistance of other countries or international organizations.
Unlike the decrease in morbidity among residents of the State of Israel following the vaccination campaign, COVID-19 morbidity and mortality rates are high among the Palestinians in the West Bank and the Gaza Strip. According to World Health Organization (WHO) data, there were 228,409 confirmed cases and 2,760 COVID-19 deaths in the West Bank as of 12 June 2021, with morbidity continuing to rise [46].

COVID-19 in the Occupied Palestinian Territories, World Health Organization (12 June 2021) [46]
COVID-19 in the Occupied Palestinian Territories, World Health Organization (14 June 2021) [46]
The local shortage of vaccines meant that the vaccination of West Bank and Gaza Strip residents only began in March 2021, three months after the commencement of the Israeli vaccination campaign. Some 272,440 vaccine doses were donated by China (SinoPharm) and the United Arab Emirates (Sputnik-V) for the 5.2 million members of the Palestinian population. In addition, the Palestinian Authority (PA) is entitled to receive vaccines for 20% of the population through the global COVAX alliance. On 7 March 2021, the Israeli government began to vaccinate over 120,000 Palestinians employed in Israel or in the settlements who are not recognized as residents of Israel[47], and 5,000 vaccine doses were delivered to PA medical staff. As of 8 April 2021, 143,142 Palestinians had been vaccinated, which represents 2.58% of the population compared to 61.32% of the population in Israel [48].
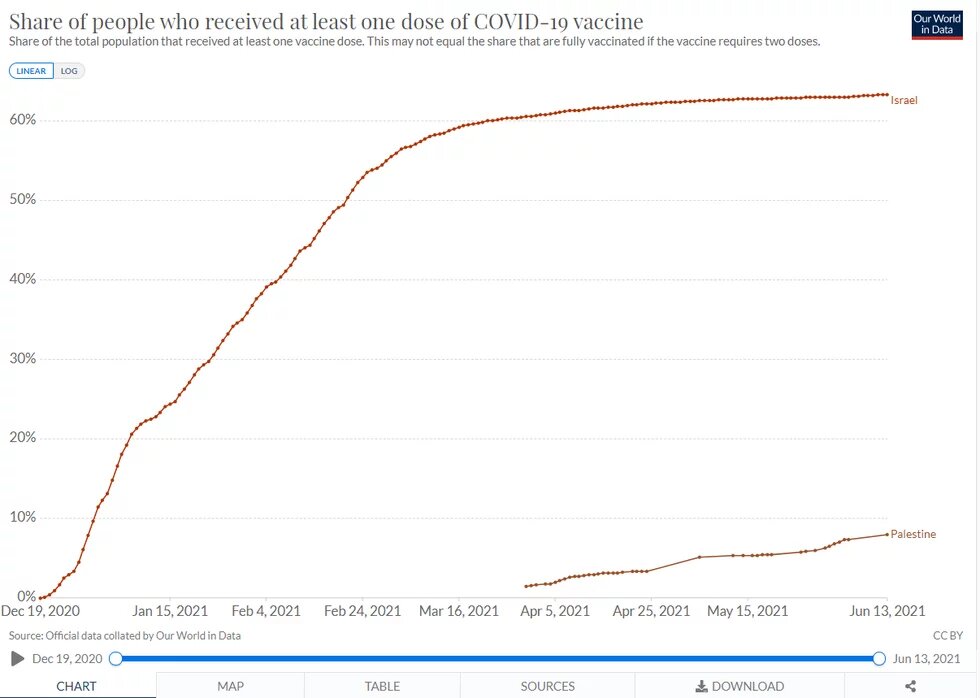
https://ourworldindata.org/covid-vaccinations (13 June 2021)
PHR-Israel contacted the Director-General of the Israeli Ministry of Health and the Coordinator of Government Activities in the Occupied Territories with the demand that vaccines be provided to the Palestinian public and the claim that Israel bears legal, ethical and humanitarian responsibility for vaccinating the Palestinian population under international law. In addition, the Israeli authorities were approached by 16 human rights organizations, including Amnesty International, that demanded that Palestinians be given vaccines that meet the Israeli standard, that is to say, not the Russian vaccine. According to these organizations, an occupying power is obliged to take the necessary precautions to prevent the spread of disease, and the fact that the PA has independently proceeded to vaccinate the Palestinian population does not absolve Israel of responsibility [49].
In a Supreme Court petition filed on 25 March 2021, PHR-Israel argued that Israel must ensure that the Palestinian population is vaccinated on moral, legal and epidemiological grounds[50]. Referring to the moral aspect, it contended that Israel bears responsibility for the residents of the territories deriving from its years-long occupation and ongoing control of the border crossings. The Gaza Strip has in effect been under siege for over 13 years, and this has exerted a ruinous impact on the territory's health system, infrastructures, and the ability to solve the problems of their overcrowded and impoverished population. As part of this responsibility, Israel must provide the Palestinians with medical solutions for dealing with the COVID-19 pandemic, including by taking steps to ensure that the population has the same access to vaccines as Israel.
In its legal arguments, PHR submitted that the International Covenant on Social, Economic and Cultural Rights of 1966 (ratified by the State of Israel in 1991) states that every person has the right to enjoy the highest attainable standard of physical and mental health (Article 12.1). The Covenant explicitly states that, for the full realization of the right to health, states must take the necessary steps to ensure the prevention, treatment, and control of communicable diseases (Article 12.2.c). Furthermore, and under Article 55 of the Fourth Geneva Convention of 1949, an occupying power must also provide for the medical needs of the occupied territory if the occupied territory’s resources are inadequate. Moreover, the right to medical treatment has been recognized in Israeli case law as deriving from the constitutional right to human dignity.
Epidemiologically, PHR claimed, the vaccination of the Palestinian population would contribute to community (herd) immunity in Israel, in the territories and in Gaza, and would reduce the danger present in the spread of variants. Furthermore, PHR argued, the SARS-CoV-2 virus does not distinguish between Israelis and Palestinians, or between one identity card and another. The numerous interfaces between the two populations make them a single epidemiological unit, and the disease will continue to afflict Israel’s citizens if there are no vaccinations in the PA.
In this respect, the petition cited a position paper published by the Israel Association of Public Health Physicians to the effect that “a uniform vaccination policy must be adopted for the citizens and residents of Israel and for PA residents, and all the more so given the fact that there is no shortage of vaccines in Israel and therefore no question of prioritization. Unless the entire population is fully or almost fully vaccinated as soon as possible, it will be impossible to eradicate the disease in the area between the Jordan River and the Mediterranean Sea with the attendant risk of the emergence of more contagious and dangerous mutations. The partial vaccination of the population will adversely impact the long- and short-term efficacy of the entire campaign, in which huge resources have been justifiably invested to save lives and to return to as normal a life as possible after a long period of restrictions and lockdowns.”
The comparison between the Israeli decline in morbidity following an impressive vaccination campaign and the continued morbidity and mortality among the Palestinian population has also prompted international criticism, with the foreign press claiming that Israel has a legal and moral obligation to transfer vaccines to the PA.
Additional pressure on Israeli policy-makers was exerted domestically [51]. Former Member of the Knesset Zehava Galon, the President of the Zulat NGO for Equality and Human Rights, wrote in this respect that “our basic humanity should spur us to raise an outcry that Gazans’ health has become a ball in a game among our cynical and brazen politicians. When we keep a vaccine from a Gazan woman who has done us no harm, we lose part of our humanity”[52]. Zulat’s Executive Director, Einat Ovadia, wrote that “Palestinian control of Areas A and B is a bad joke. These areas are enclaves within territories under Israeli control.... Israel is strong enough to allow the Palestinians to get vaccinated, even if this hurts Netanyahu at the ballot box”[53].
In January 2021, Zulat declared its public support for a petition, also signed by its president, which called on Israel to provide vaccines to the Palestinians under its control in the West Bank and Gaza Strip [54]. The Zulat Human Rights Index published in March 2021, which surveyed the views of Israelis regarding Israel’s obligation to provide vaccines to the Palestinians in the Occupied Territories, showed that 46% of all respondents were in favour of doing so [55].
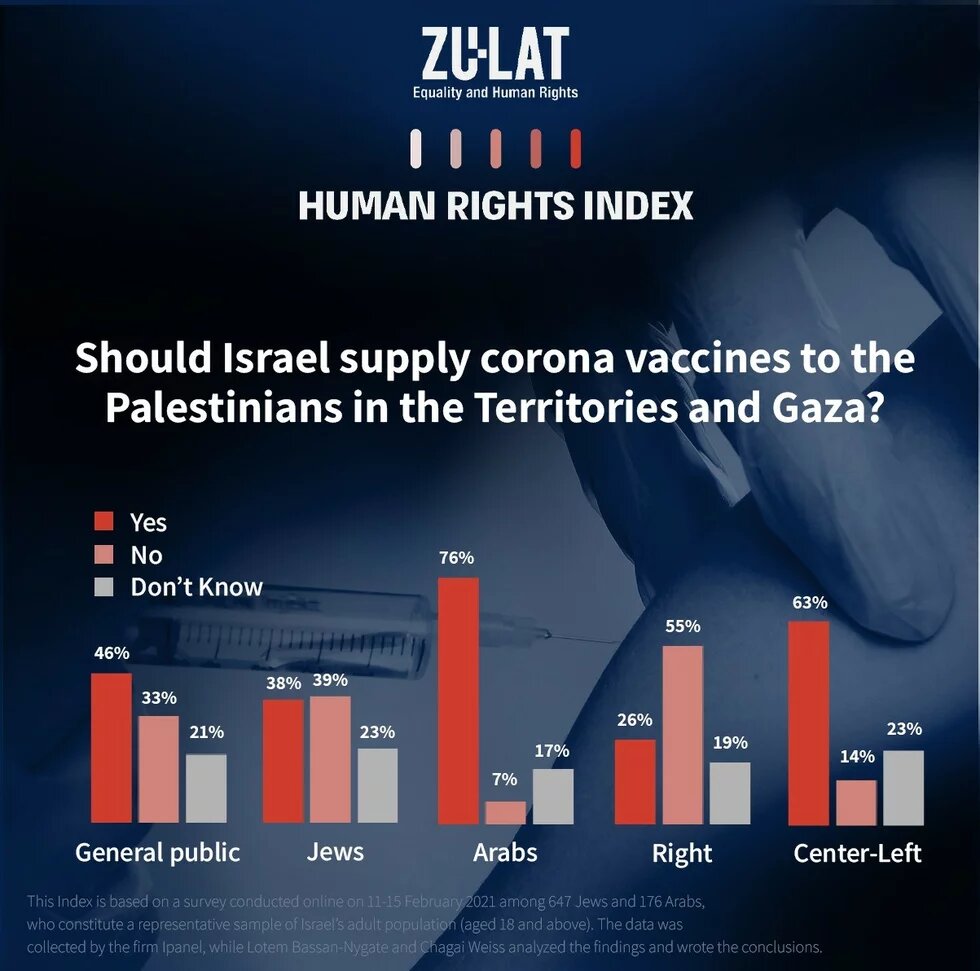
https://zulat.org.il/en/activities/human_rights_index_feb21/ [55]
The Israeli government, however, maintains that the State of Israel has no legal obligation to vaccinate the Palestinian population in the West Bank and Gaza Strip. This position is based on the Israeli-Palestinian Interim Agreement of 1995, under which civilian powers, including the health of the Palestinian population, were transferred to the PA. However, conventional wisdom suggests that Israel should be interested, from both a health standpoint as well as politically, in having the Palestinians vaccinated in the same way as Israeli residents.
Accordingly, Israel began transferring vaccines meant for medical personnel to the PA in February 2021. In addition, the residents of East Jerusalem and PA residents working in Israel were entitled to be vaccinated in Israel [56]. In March 2021, it was announced that Israel had transferred 64,000 vaccine doses funded by Pfizer and the WHO to the PA. However, the amount of vaccines at the PA’s disposal is insufficient for vaccinating the entire Palestinian population and all official bodies in Israel (including the Ministry of Defense and the Ministry of Health) recommend that Israel help the Palestinians obtain more vaccines. Such assistance is undoubtedly urgently required in light of the severe morbidity in both the West Bank as well as the Gaza Strip [57].
In addition to their stated support for the position that Israel bears responsibility for vaccinating the Palestinian population, Israeli human rights organizations (Zulat and PHR) also voiced an opinion with regard to the responsibility borne by the WHO [58], affirming that one of the its most important functions is to stop the outbreaks of epidemics. The WHO has led a widely publicized and successful global effort that sought to make childhood immunization accessible to the world’s poorest countries, to eradicate smallpox and to stamp out polio.
A similar effort built on cooperation and meant for ensuring that all countries have access to vaccines is now needed for dealing with COVID-19. Equitable access is essential in light of both the universal right to health as well as the global economic costs exacted by the pandemic. To this end, measures are necessary for overcoming the obstacles to equality and fairness in access to vaccines by the current patent regime, whether via the willingness of governments and pharmaceutical companies to voluntarily share knowledge, or via an initiative similar to that established by India and South Africa that suspends vaccine manufacturers’ patent licenses temporarily [59].
How have political alliances played out in the vaccination context?
In February 2021, it was announced that Israel’s Prime Minister and National Security Council (NSC) had decided to transfer thousands of Moderna vaccines to a list of 18 countries: Sudan, Morocco, Mauritania, Chad, Congo, Equatorial Guinea, Uganda, Niger, Kenya, Ethiopia, Honduras, Guatemala, Italy, Cyprus, San Marino, Hungary, the Czech Republic and the Maldives. Some of these countries had tightened relations with Israel in recent years, including: Guatemala, which moved its embassy to Jerusalem in 2018, Honduras, which has announced its intention to do the same, and the Czech Republic, which has stated its willingness to open a “diplomatic office” in Jerusalem in addition to its embassy in Tel Aviv.
The aforementioned decision was said to have been made for humanitarian reasons, as well as with a view to boosting relations and deepening the friendly ties with countries that have stood by Israel in the past [60]. According to Israeli Prime Minister Benjamin Netanyahu, “these are symbolic quantities. This is an informed decision in exchange for many rewards we have received in various fields.” However, the decision also attracted domestic criticism, as it was made without prior consultation with the Ministry of Defense, the Ministry of Health or the Ministry of Justice. The decision was later suspended after the Attorney General of Israel requested an explanation from the director of the NSC.
In March 2021, Israel received an exceptional U.S. request to transfer 2,400 vaccine doses to the multinational force (MFO) in Sinai in order to vaccinate the staff and soldiers stationed there as part of the Israel-Egypt peace treaty. The MFO is expected to bear the cost of the vaccines and their transportation. Unlike the earlier 18-country decision, the American request was discussed by the Ministry of Defense and deemed justified on diplomatic and security grounds [61].
Conclusion
Which recommendations should be made? How can countries in the Global North help in ensuring a just and equitable vaccination?
In order to ensure fairness in the vaccination campaign, international support for an initiative similar to that of India and South Africa is required so that the vaccine manufacturers’ patent licenses are suspended until the pandemic is eradicated.
On a national level, vaccines should be purchased and supplied exclusively by the state in order to prevent people of means from “jumping the line”. They should also be provided free of charge to the entire population, including asylum seekers and visa-less migrant workers, and without neglecting geographical and social peripheries.
In terms of prioritization, the vaccination campaign should prioritize the population at risk of serious illness and the staff coming into contact with them. Furthermore, a logistical apparatus should be established for the vaccination of homebound elderly persons living in the community and their caregivers, which should be similar to the one established for caregivers in long-term nursing facilities. Prioritization decisions should also be made by an apolitical professional committee made up of experts in various fields and drawn from diverse sectors of the population.
As for dealing with “vaccine hesitancy”, this requires the active monitoring (including on social media) of the issues worrying the public and a respectful response to them. Information about the vaccine and about vaccination should be adapted to different populations and sectors, and opinion influencers in the various communities should be enlisted to this end. In light of the great weight that the public attaches to their position and opinions, medical staff should also be provided with comprehensive information and guidance on how to present information on the vaccine to patients and on how to encourage vaccination.
The full disclosure of existing information about vaccines and transparency at all stages of decision-making should be ensured in order to promote public trust. This should include explaining the reasons for decisions, maintaining consistency, avoiding conflicts of interest and encouraging public participation. Given research findings that indicate that the vaccine reduces infection (as well as the risk of illness), there is also a need for emphasizing the importance of the vaccine in providing protection at the public level rather than at the personal level alone.
Insofar as vaccinated people are allowed to enter businesses and public places, a similar prerogative should be given to those who cannot be vaccinated due to contraindications, as well as to people presenting a positive serological test or a negative COVID-19 test. Having said that, a mandatory proof of vaccination requirement must be avoided in places where entry is essential for the exercise of basic rights: hospitals, clinics, pharmacies that ensure the right to health or houses of worship that ensure the freedom of worship. Making the entry of employees into their workplaces contingent on providing proof of vaccination or on presenting a negative COVID-19 test should only be carried out in cases where such a measure would be imperative for safety reasons, such as when physical distancing is impossible due to the type of work conducted at a given workplace or when the work conducted in a workplace involves contact with at-risk populations such as children (who are currently contraindicated) or elderly persons (who may be less immune despite being vaccinated).
All in all, the pursuit of the common good and a commitment to social justice are what will lead to fairness in the vaccination of the population at both the global and national levels.
References
- Ministry of Health, Flight from Italy with COVID-19 Patient, 27 February 2020
- I24 News, Israel To Impose Passover Lockdown Amid Pandemic, 7 April 2020
- BBC News, Coronavirus: Israel To Impose Three-Week National Lockdown, 13 September 2020
- Ministry of Health, COVID-19 Vaccine Operation Launched Today, 19 December 2020
- Ministry of Health, Data Dashboard, cited 11 April 2021
- US Food & Drug Administration, Pfizer-BioNTech COVID-19 Vaccine, cited 11 April 2021
- Sheba Medical Center, Human Trials of Israeli COVID-19 Vaccine to Begin at Sheba, cited 11 April 2021
- Coherent Market Insights, COVID-19 Vaccine Tracker
- Ahronheim A., What Is the Secretive Institute That Found an Antibody to Coronavirus?, The Jerusalem Post, 6 May 2020
- The Jerusalem Post, Participants in Israeli-Made Vaccine Trials Not Eligible for Green Pass, 4 March 2021
- Ministry of Health, Cabinet Approves Health Ministry Regulations for Third Phase That Will Begin Sunday, 7 March 2021, 6 March 2021
- Globes, Israel Signs Agreement for 4m. More Moderna Vaccine Shots, 6 December 2020
- Rosen, B., Waitzberg, R., Israeli, A., Israel's Rapid Rollout of Vaccinations for COVID-19, Israel Journal of Health Policy Research, 26 January 2021.
- Weinerb G., Israel Changed Plans to Buy AstraZeneca Vaccine, Globes, 25 November 2020
- Israeli Online Legislation Database, National Health Insurance Law, accessed April 2021 (Hebrew)
- AFP and TOI Staff, How Israel's Efficient, Data-Savvy HMOs Help It Lead World in COVID Vaccination, The Times of Israel, 13 January 2021
- Pharmacists' Regulations (Medical Preparations) 1986, Regulation 29 (9), Nevo Database (Hebrew)
- Ministry of Health, Real World Epidemiological Evidence Collaboration Agreement
- Jaffe-Hoffman M., Where Are Israel's Moderna Vaccines?, The Jerusalem Post, 14 February 2021
- Yaron L., Tel Aviv Launching COVID Vaccine Campaign for Asylum Seekers, Haaretz, 8 February 2021.
- Caspi G., Dayan A., et al, Socioeconomic Disparities and COVID-19 Vaccination Acceptance: Experience from Israel, Medrxiv Preprint, 1 February 2021
- Daoud N., Vaccinations Need to Be Made Accessible If the Arab-Israeli Population Is to Be Vaccinated, Globes, 20 January 2021 (Hebrew)
- Ashkenazi S., Israeli Health Ministry Sets Vaccination Priorities, Globes, 10 December 2020
- Adalah-The Legal Center for Arab Minority Rights in Israel, Israeli Minister Blocks COVID-19 Vaccinations for Palestinian Prisoners; Adalah Demands Decision Be Overturned, 28 December 2020
- Breiner J., High Court Strikes Down Public Security Minister's Order to Withhold Vaccines From Prisoners, Haaretz, 1 February 2021
- Ministry of Health, Recommendation That Pregnant Women with Frequent Exposure to People with Chronic Medical Conditions Get Vaccinated, 19 January 2021
- The Guardian, Vaccinating Women Who Are Planning Pregnancy, Pregnant or Breastfeeding with COVID-19 Vaccine - Clarification, 28 January 2021
- Holmes O., Israel Opens Coronavirus Vaccines to All Over-16s, The Guardian, 3 February 2021.
- Israeli Pediatric Society and Infectious Disease in Children Organization, Position Paper: Vaccination Against COVID-19 of Children Between the Ages of 12 and 15, 13 April 2021 (Hebrew)
- Bank of Israel, Research Department Forecast, January 2021, 4 January 2021
- Bank of Israel, Research Department Forecast, April 2021, 19 April 2021
- Green M.S., Abdullah R., Vered S., et al, Study of Ethnic, Gender and Educational Differences in Attitudes Toward COVID-19 Vaccines in Israel – Implications for Vaccination Implementation Policies, Israel Journal of Health Policy Research, 19 March 2021
- Velan B., Vaccine Hesitancy as Self-Determination: An Israeli Perspective, Israel Journal of Health Policy Research, 4 April 2016
- Dror A. A., Eisenbach N., et al, Vaccine Hesitancy: The Next Challenge in the Fight Against COVID-19, European Journal of Epidemiology, 12 August 2020
- Kavaler T., Israel's Experts Fear 'Fake News' Harming Vaccine Drive, Ynetnews, 5 March 2021
- Rosner Y., 20 Years Since October 2000: Structural Health Discrimination Between Arabs and Jews, Physicians for Human Rights, 3 November 2020
- Boxerman A., Officials Concerned by Low Vaccination Rate Among Arab Israelis, The Times of Israel, 31 December 2020
- Boxerman A., Arab Israelis Fret Over Lagging Vaccination Rates as Ramadan Approaches, The Times of Israel, 8 March 2021
- Zulat and Physicians for Human Rights-Israel, The Right to Vaccination - Confronting Vaccine Hesitancy, 2 April 2021 (Hebrew)
- State Comptroller's Office, State Comptroller Report: Children, Adults and Healthcare Workers' Immunization, 2014 (Hebrew)
- Ministry of Health Summary Report on Health Services for Students in the 2019-2020 Schoolyear, (Hebrew)
- Ministry of Health, COVID Fake News, cited 22 April 2021
- TOI Staff, Health Ministry Sets Up Team to Fight Fake News on Vaccines, The Times of Israel, 14 February 2021
- Scharf I., Ben Zion I., As Vaccinations Lag, Israel Combats Online Misinformation, AP News, 15 February 2021
- Sokol S., Arab-Israelis Lag Behind in Israel's Vaccination Success Story, Forward, 16 February 2021
- World Health Organization, Coronavirus Disease in the Occupied Palestinian Territory, 17 April 2021
- United Nations Office for the Coordination of Humanitarian Affairs, COVID-19 Emergency Situation Report 29: March 2021, 12 April 2021
- Ritchie T., Ortiz-Ospina E., et al, Coronavirus (COVID-19) Vaccinations, University of Oxford, cited 22 April 2021
- Shusterman N., The Palestinians and COVID-19 Vaccines: An Israeli Responsibility?, Institute for National Security Studies, 2 February 2021
- Gisha, Supreme Court Petition: Physicians for Human Rights-Israel v. The State of Israel, 25 March 2021 (Hebrew)
- Kamin-Friedman S., Israel Has Moral Duty and Health Need to Vaccinate Palestinians, Ynetnews, 12 January 2021
- Galon Z., Gaza, COVID Vaccines and One of the Most Disgraceful Hearings Ever Held by Knesset, Haaretz, 18 February 2021
- Ovadia E., The Oslo Accords' Flak Jacket, The Times of Israel, 25 February 2021 (Hebrew)
- Galon Z., One Person's Life Is Not Worth More Than Another Person's Life. Israel Must Provide Vaccines to Palestinians Under Its Control in the West Bank and Gaza, Twitter, 12 January 2021
- Zulat, Human Rights Index, 11 March 2021
- Boxerman A., Israel To Send Palestinians 5,000 Coronavirus Vaccine Doses for Health Workers, The Times of Israel, 31 January 2021
- BBC News, COVID-19: Palestinians Lag Behind in Vaccine Efforts as Infections Rise, 22 March 2021
- Kamin-Friedman S., The Right to Vaccination: Policy Paper by Zulat and Physicians for Human Rights-Israel, 8 January 2021
- World Trade Organization, Communication from India and South Africa: Waiver from Certain Provisions of the TRIPS Agreements for the Prevention, Containment and Treatment of COVID-19, 2 October 2020
- Kingsley P., Israel Gives Vaccine to Far-Off Allies, As Palestinians Wait, The New York Times, 23 February 2021
- Cohen G., Israel Renews Vaccine Diplomacy, Kan-Israeli Broadcasting Corporation, 8 March 2021 (Hebrew)